

Avoidant/Restrictive Food Intake Disorder (ARFID) has gained some recognition and traction over the past couple years, and we are still continuing to learn more and more as research continues. There’s a few ways ARFID can present, which we’ll get into below, but ARFID is an eating disorder characterized by an extreme avoidance of certain foods or a severely restricted diet.
ARFID is much more than “picky eating”, it is an eating disorder that affects adults and children, though it is most commonly diagnosed in childhood. ARFID can be broken up into 3 different types: avoidance of foods or food groups due to sensory sensitivities such as certain textures, fear of negative consequences, or a lack of interest in eating.
ARFID is commonly thought to not be associated with any body image concerns or negative consequences associated with food, and while that may be true for the majority of those who struggle with ARFID, that is not always the case. Ignoring this nuance can prohibit someone from getting proper treatment.
ARFID is often described as having three primary subtypes based on the underlying causes of food avoidance and restriction. It is possible to meet criteria for more than one subtype, too!
Individuals with this subtype typically avoid foods based on sensory characteristics such as taste, texture, color, or smell. Sensory consistency can be a big part of this subtype, and whether or not a food is always going to be slimy, crunchy, etc. Let me give you an example I often share with patients/caregivers. A blueberry can have many different characteristics: juicy, sour, sweet, big, small, mushy, etc.
Now compare that to a cheese-it, where it’s most often always going to have the same characteristics. There is no question of what texture, taste, smell, or color the cheese-it is going to have. For people who struggle with sensory sensitivity, It is very common to gravitate towards carbohydrate foods such breads, crackers, pastas, rice, etc. because these are foods that are often most consistent.
Foods such as vegetables, fruits, and proteins often have the most potential changes in sensory characteristics, which is why they’re often avoided. Changes in sensory sensitivity can cause anxiety and make eating experiences much more difficult.
This subtype involves an overwhelming fear and anxiety that eating certain foods will result in negative physical outcomes, such as choking, vomiting, or stomach pain. For example, a child may develop a fear of eating after experiencing a choking incident or stomach illness.
As a result, those with this type of ARFID may avoid eating altogether or restrict themselves to foods that they believe are safe. This can also extend to seeing someone else choke or get sick from a food, and not just relate to the person themselves. The fear of adverse consequences can severely limit food choices over time, which can lead to food restriction that significantly impacts nutritional intake and growth and development, especially in children.
This subtype is characterized by a general lack of interest in food. People with this form of ARFID may simply not feel hungry or may be indifferent to the act of eating. Food is sometimes labeled as a chore, which can make responding to hunger cues (if they are present) much more difficult. They may not experience the urge to eat as others do, which can cause significant weight loss or malnutrition if left untreated.
While the exact causes of ARFID remain unclear, a combination of biological, psychological, and environmental factors may contribute to developing ARFID. Some possible factors include:
Treatment for ARFID can be complex, as it involves not only addressing restrictive eating patterns but also tackling the psychological and sensory issues that contribute to food avoidance. Eating disorder treatment is tailored to the individual’s needs and may involve a combination of therapies and interventions:
CBT can help individuals identify and challenge negative thoughts and behaviors related to food. For example, a therapist may work with a patient to address their fear of choking or vomiting, helping them reframe these fears and gradually reintroduce avoided foods. CBT can be helpful in building coping strategies for anxiety around sensory issues and therefore improve eating behaviors.
Exposure therapy is often used in conjunction with CBT to help individuals gradually confront their food aversions in a controlled and safe manner. By slowly and systematically exposing individuals to feared foods or eating situations, the therapist and/or registered dietitian can help build distress tolerance around anxiety-producing stimuli.
One thing to keep in mind is that challenging foods/food exposures may not always be something the patient wants to do, and as their provider we have to listen to them. In that case, the goal would be to make sure they are eating enough for their body’s needs.
Working with a registered dietitian can help ensure that individuals with ARFID are getting the proper nutritional intake to support their body to prevent malnutrition. That may be 100% through safe foods, and that’s okay! Vitamin/mineral supplements can be helpful when micronutrient needs may not be getting met through food. This just helps to avoid any deficiencies. The dietitian can also be a crucial part in food exposure planning and helping to identify what foods the patient is wanting to try.
Some gentle reminders:
For children and adolescents with ARFID, family involvement can be crucial in the treatment process. Family-based therapy focuses on educating parents, providing them with strategies to support their child, and helping the family work together to create a sustainable relationship with food.
Due to the restrictive nature of ARFID, medical intervention may be needed to ensure there are no vitamin/mineral deficiencies, address any growth concerns, monitor weight if warranted, and ensure stability.
Neurodivergence is a term for individuals whose brain is different from what is seen as “typical” and allows people to think, learn, and interact with the world differently. People who are neurodivergent often report sensory sensitivity to certain foods, which can also impact how someone experiences hunger and subsequently impacts how they feed their body.
This can be tricky when trying to identify someone’s hunger cues (because it’s not always a stomach growl), and why honoring hunger cues isn’t always a part of this work. Sometimes feeding and eating has to be more prescriptive, meaning that there may need to be more of a plan for meals/snacks vs someone waiting for hunger cues (because they may never come).
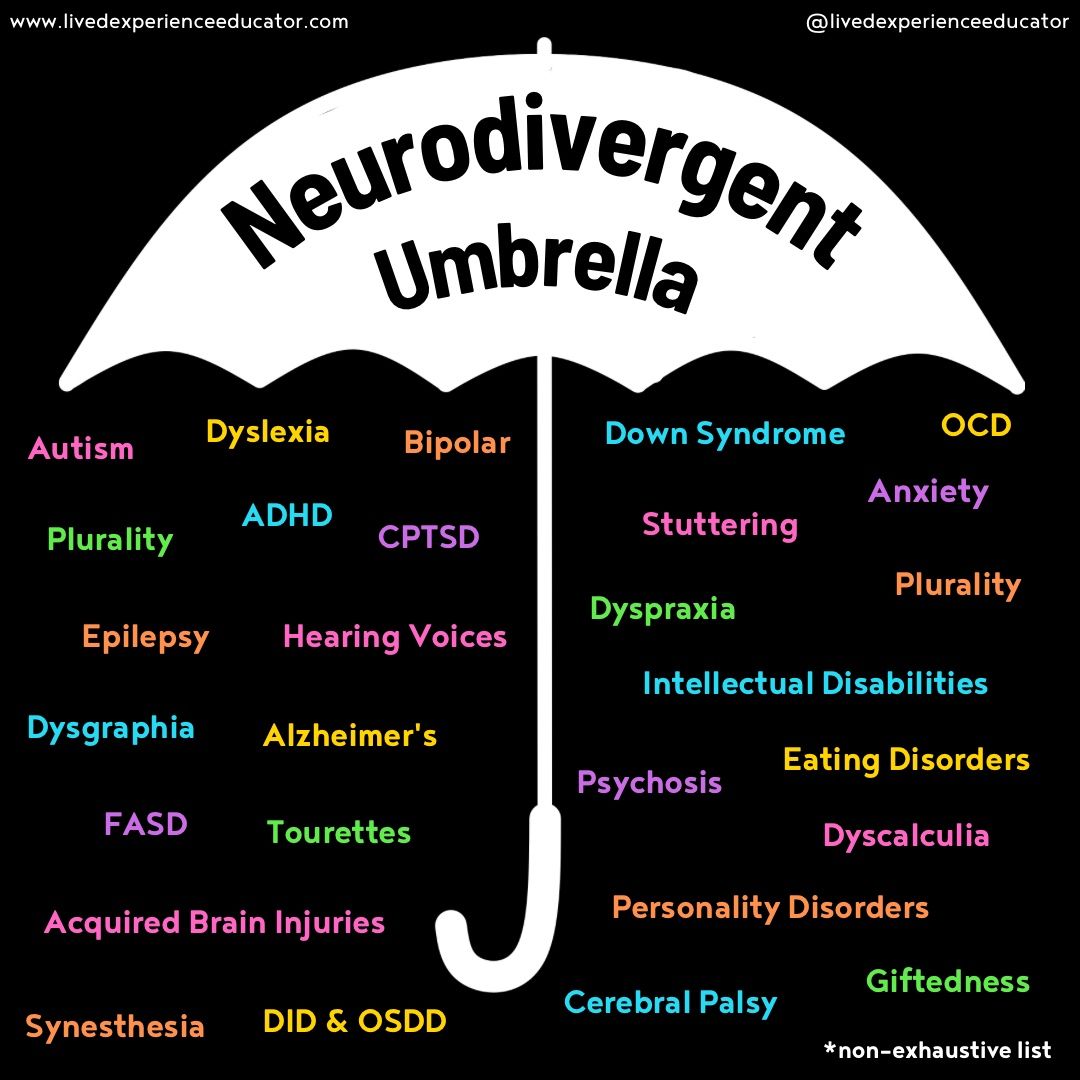
Although research on eating disorders and neurodivergence continues to remain limited, there is a connection between people with neurodevelopmental differences such as autism, ADHD, and intellectual differences, and eating disorders. If you look at the umbrella, eating disorders also fall under neurodivergence.
Specifically for people diagnosed with ARFID, over half will have a neurodivergence, psychiatric, or somatic diagnosis, and of the children diagnosed with ARFID, 8.2-54.% are also autistic. Another study found that 16.27% of those diagnosed with ARFID are also diagnosed with autism. Why is this important? People with autism and other spectrum disorders often experience sensory sensitivity to not just food, but clothing, lighting, sound, and smells.
This does not mean that all people who have ARFID will also have autism or sensory sensitivity, but it’s important to recognize the connection and how it could potentially impact how someone is able to feed themselves.
As you can see, ARFID is much more complex than “picky eating”, and often requires a nuanced approach to treatment. This work requires compassionate care, and If you think you or someone you know may be navigating ARFID, you deserve to be seen and seek help.
References:

Hi! I’m Jordyn (she/her), a Registered and Licensed Dietitian Nutritionist who specializes in eating disorders. I work with both adolescents and adults to find freedom from food and peace with their bodies from a non-diet, weight-inclusive, Health At Every Size (HAES) approach. I’ll help provide a safe & non-judgmental environment so that you always feel safe when sharing about your relationship with food and your body. I’ll help you find enjoyment and connection in food again (because food is meant to be enjoyed) and a healing relationship with your body, however that looks for YOU, because there is no cookie-cutter definition of recovery.

Weight-inclusive and trauma-informed nutrition and therapy services.

Copyright © 2026. A Soft Place to Land. All rights reserved.
